When it comes to interpreting visual fields, one of the more subtle aspects of visual fields is distinguishing between absolute scotomas and relative scotomas. On the surface, this may seem fairly simple; on a grayscale readout, absolute scotomas tend to be completely black, while relative scotomas are varying shades of lighter gray. However, some relative scotomas can still look fairly dense.
Another helpful feature is how “steep” the visual field is: on an automated visual field test, the output will show an area of normal sensitivity next to an area that is markedly decreased. For example, the output might show points with normal sensitivity (30 dB) next to points of <0 dB, or the depression may be less prominent, such as 15 dB.
For visual field defects secondary to neurological diseases, a rule of thumb that may be helpful in considering potential etiologies for the visual field defects is that vascular lesions tend to have steeper defects than compressive lesions (tumors).
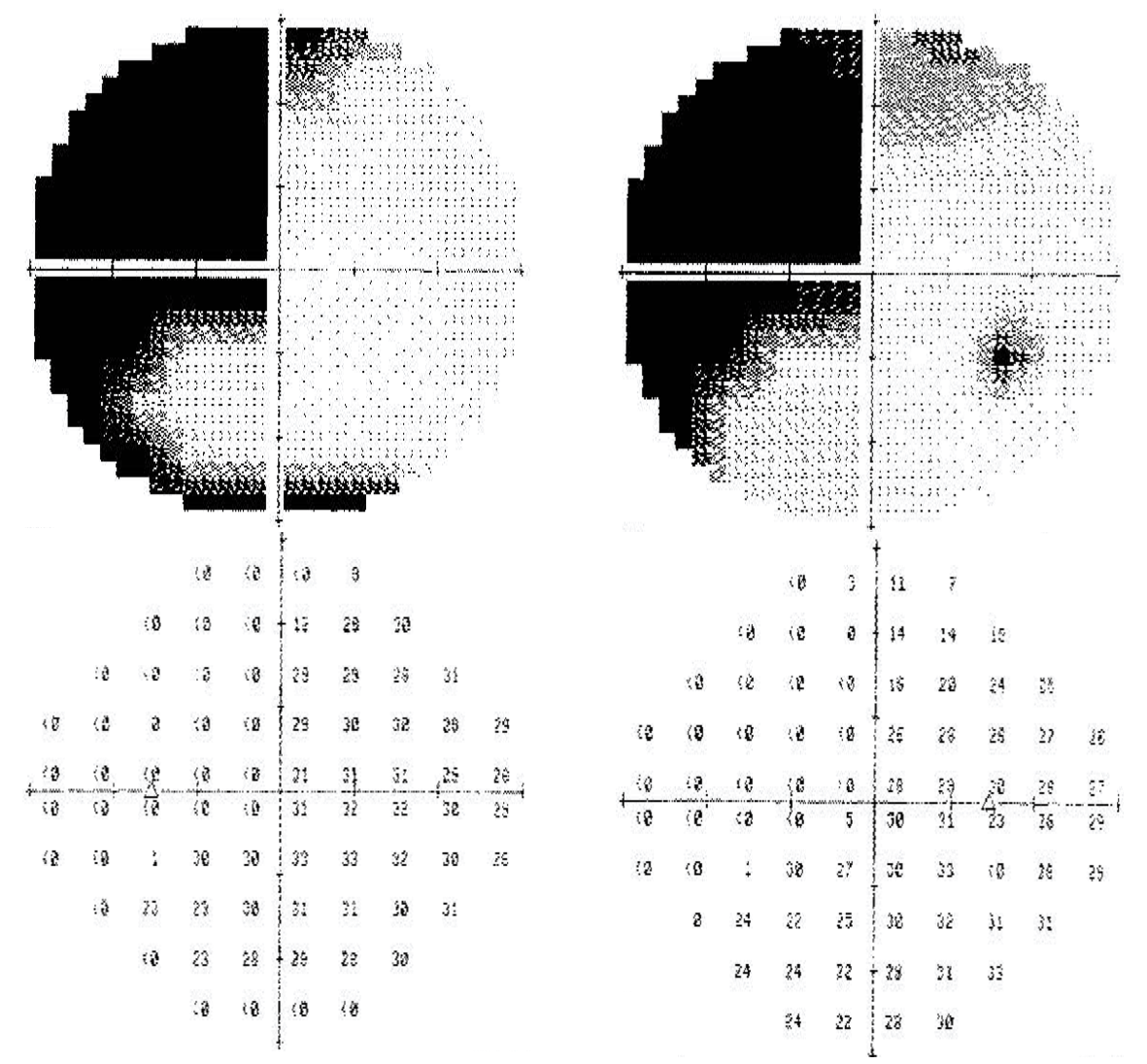
Left homonymous hemianopia (stroke). Note that the left superior quadrant in each eye has a sharp decrease in the sensitivity between the non-seeing area and the seeing area.
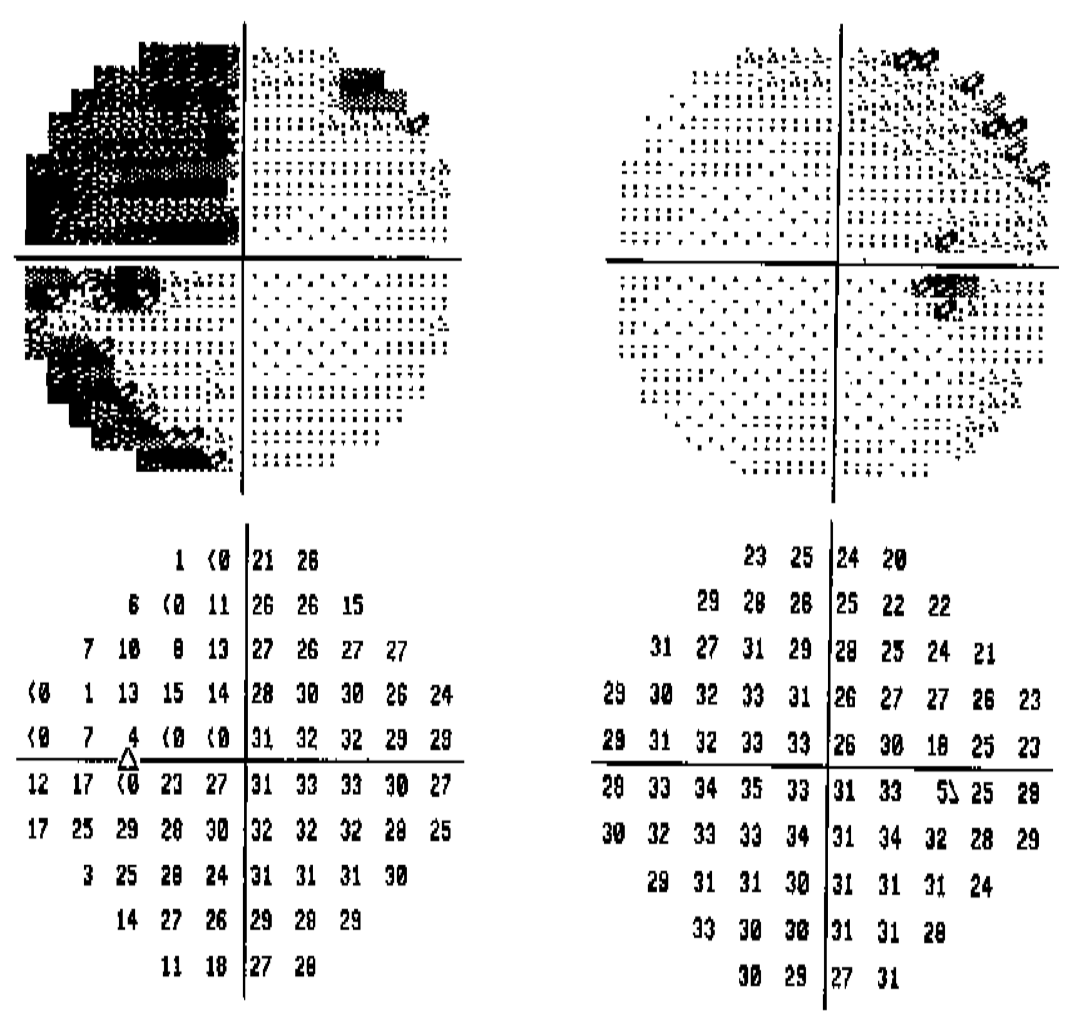
Bitemporal hemianopia, left worse than right (pituitary adenoma). Note that visual field loss still respects the vertical midline but the depression is not as severe compared to the loss in a stroke.
Reference
Walsh TJ, ed. Visual Fields: Examination and Interpretation. Third Edition. New York: Oxford University Press, 2011: 6.