I'm going to shift gears a little bit and start reviews on some of the other sections. I originally had planned to go in order of the BCSC sections and follow the OKAP content outline, but I realized that of all the sections to cover, General Medicine is one of the smallest sections in terms of content to know. So while I will likely get back to it sometime in the future, I wanted to make sure the key subjects were discussed prior to the test.
There are many facts in the Fundamentals and Principles of Ophthalmology section of the BCSC that will likely be tested as quick recall. I promise, I will eventually provide numerous resources and tools to help remember these facts; for this article, I will try to cover the most important concepts. I am intentionally leaving out details that may be more challenging to test (meaning I have a hard time coming up with a practice question about it).
Orbital Anatomy

Image credit: AccessLange: General Ophthalmology. Available online at Oculist.
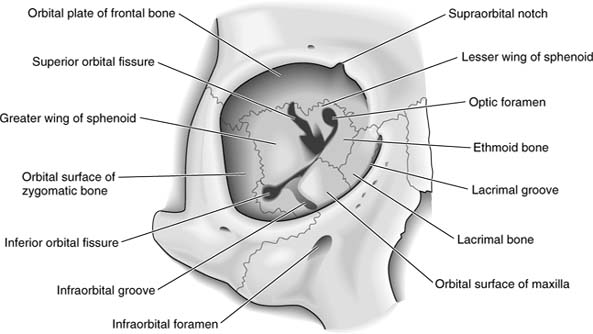
Bones of the Orbit
There are 7 bones that make up the orbit (in no particular order):
- Ethmoid
- Lacrimal
- Frontal
- Sphenoid
- Maxillary
- Palatine
- Zygomatic
Check out our article on the orbital bones for more details.
Orbital Roof
- The orbital roof consists of two bones: the frontal and sphenoid bone (lesser wing).
- The frontal bone contains the lacrimal gland fossa temporally and the trochlear fossa nasally.
Lateral Orbital Wall
- The lateral orbital wall consists of two bones: the zygomatic and the sphenoid bone (greater wing).
- The lateral orbital wall is the strongest wall of the orbit.
Orbital Floor
- The orbital floor consists of three bones: the palatine, the zygomatic, and the maxillary bones.
- The lacrimal fossa is formed by the maxillary and lacrimal bones, which contains the nasolacrimal duct.
- The inferior oblique muscle originates from the orbital floor, lateral to the nasolacrimal duct.
- The orbital floor is the only wall of the orbit that does NOT contain part of the sphenoid bone.
- The orbital floor is the most frequently fractured wall in trauma where an object larger than the orbit (such as a ball or fist) impacts the entire orbit. Typically the orbital rim is not fractured, as the impact force is distributed throughout the entire orbit, inducing a floor fracture (orbital blowout). In some extreme cases, the fracture can extend to the medial orbital wall.
Medial Orbital Wall
- The medial orbital wall consists of four bones: the sphenoid (lesser wing), maxillary, ethmoid, and lacrimal bones.
- The medial orbital wall is the thinnest wall of the orbit; the lamina papyracea is the paper-thin aspect of the medial orbital wall.
- Sinus infections can spread to the orbit through the medial orbital wall.
Whitnall's Tubercle
Whitnall's tubercle is a prominence along the zygomatic bone. It serves as the attachment for several key soft-tissue structures (the "4 L's"):
- Lateral rectus check ligament
- Lateral palpebral ligament
- Lockwood suspensory ligament
- Levator aponeurosis
Please see our article on Whitnall's tubercle for more detailed information.
**Note: Whitnall's ligament does NOT attach to Whitnall's tubercle...(if you believe what they say on the Internet)
Nasolacrimal Duct
- The nasolacrimal duct originates at the lacrimal fossa and drains into the inferior meatus.
- In dacryocystorhinostomy, the nasolacrimal duct is bypassed and a new drainage opening (ostomy) is formed between the lacrimal sac and the middle meatus.
Fissures
Superior Orbital Fissure
The superior orbital fissure contains many key structures. They are typically organized into structures above the annulus of Zinn and those within the annulus of Zinn.
One of the many reasons why these distinctions are important is because retrobulbar blocks are theoretically intraconal; therefore, structures within the annulus of Zinn will be affected by the block, whereas structures outside the annulus will not.
Structures ABOVE the annulus of Zinn:
- Lacrimal nerve (branch of CN V1)
- Frontal nerve (branch of CN V1)
- Trochlear nerve (CN IV)
- Superior ophthalmic vein
Structures WITHIN the annulus of Zinn:
- Oculomotor nerve (CN III, superior and inferior divisions)
- Nasociliary nerve (branch of V1)
- Sympathetic nerves
- Abducens nerve (CN VI)
Inferior Orbital Fissure
There are 4 major structures that pass through the inferior orbital fissure:
- Infraorbital nerve (branch of V2)
- Zygomatic nerve (branch of V2)
- Nerves from the pterygopalatine ganglion
- Inferior ophthalmic vein: venous drainage will be discussed later, but the inferior ophthalmic vein drains into the pterygoid plexus, which drains into the cavernous sinus.
Sample Questions (answers at the bottom of the page)
- Which of the following bones is part of the orbital floor?
A. Frontal bone
B. Ethmoid bone
C. Palatine bone
D. Sphenoid bone
- Which orbital wall does NOT contain the sphenoid bone?
A. Orbital roof
B. Lateral orbital wall
C. Orbital floor
D. Medial orbital wall
- Which of the following structures does NOT attach to Whitnall's tubercle?
A. Lateral rectus check ligament
B. Superior transverse ligament
C. Inferior suspensory ligament
D. Lateral palpebral ligament
- Which of the following structures lies outside the annulus of Zinn?
A. Oculomotor nerve (CN III)
B. Frontal nerve (CN V1)
C. Nasociliary nerve (CN V1)
D. Sympathetic nerves
Eyelid Anatomy
The eyelid structures are divided into anterior and posterior lamellae by the orbital septum.
Anterior Lamella
Skin
- Eyelid skin is the thinnest in the body.
- It contains cilia, sebaceous glands, and sweat glands.
- The superior eyelid fold is formed by attachments from the levator aponeurosis. Asians do not have this attachment, and thus do not have superior eyelid folds.
- The levator palpebrae superioris has its firmest attachments along the anterior aspect of the tarsus, 3 mm superior to the eyelid margin.

Histology of eyelid skin at the margin. Superiorly the keratinized squamous epithelium covers the orbicularis muscle. Note the hair follicles and glands, present within the epithelial and subepithelial layers. Posterior to the orbicularis muscle lies the orbital septum, with the conjunctival epithelium forming the posterior aspect of the eyelid. The muscle of Riolan, an extension of the orbital segment of the orbicularis ocular muscle which forms the gray line of the eyelid margin, is seen at the far right aspect of the slide.
Image credit: StudyBlue.
Eyelid Margin
- The eyelid margin consists of the following structures (from anterior to posterior):
- Cilia
- Gray line (intermarginal sulcus): the gray line represents the muscle of Riolan, the most superficial aspect of the orbicularis oculi. It arises from the orbital division of the orbicularis oculi.
- Meibomian gland orifices
- Mucocutaneous junction
- The cilia are surrounded by the sebaceous glands of Zeis ("Zeibaceous" glands).
- Sweat glands on the eyelid skin are apocrine and are called Moll glands.
- The puncta, which form the point of entry for tear drainage, are slightly asymmetric. The inferior puncta are positioned slightly more lateral (6.5 mm from medial canthus) than the superior puncta (6.0 mm from medial canthus).
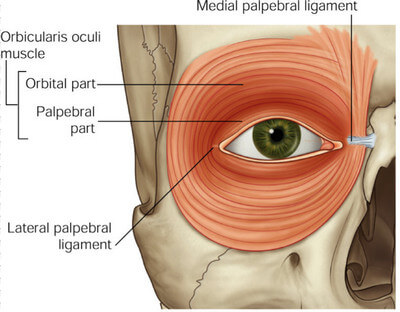
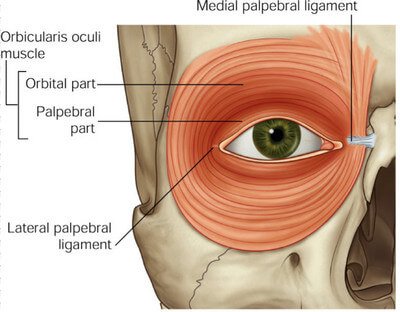
Orbicularis Oculi Muscle
- The orbicularis oculi muscle is innervated by the facial nerve (CN VII). The motor endplates are spread along the entire muscle, which allows a focal subcutaneous injection of Botox to distribute along the entire muscle.
- There are two portions of the orbicularis oculi muscle: the orbital and palpebral segments.
- The orbital segment consists of purely voluntary muscle fibers. These fibers are responsible for forced closure of the eyelids.
- The muscle of Riolan, which forms the gray line of the eyelid margin, arises from the orbital segment of the orbicularis oculi muscle.
- The palpebral segment consists of both voluntary and involuntary muscle fibers. The palpebral segment is responsible for the blink reflex.
- The palpebral segment is divided into the pretarsal and preseptal segments.
- Horner's muscle, which is a part of the pretarsal orbicularis, attaches to the anterior and posterior lacrimal crest, which creates a pumping effect for tears to drain into the puncta.
{kind=link}
{kind=link}
The orbicularis oculi muscle.
Image credit: healthfixit.com.
{kind=link}
Orbital Septum
- The orbital septum separates the anterior lamella from the posterior lamella.
- It is an extension of the periosteum.
- It serves as a protective barrier to the spread of infection and inflammation from structures anterior to the septum ("preseptal cellulitis").
- It attaches inferiorly to the anterior surface of the tarsus, anterior to the levator aponeurosis and Müller muscle.
Posterior Lamella
Levator Palpebrae Superioris Muscle and Aponeurosis
- The levator palpebrae superioris muscle arises from the lesser wing of the sphenoid bone, just superior to the superior rectus muscle.
- The muscle is innervated by the superior division of cranial nerve III.
- Whitnall's ligament (superior transverse ligament) changes the direction of pull of the levator palpebrae from horizontal (anterior-posterior) to vertical (superior-inferior).
- At the level of Whitnall's ligament the palpebral segment of the levator palpebrae superioris splits into an anterior and posterior division:
- The anterior division is the levator aponeurosis. It divides the lacrimal gland into the orbital and palpebral lobes. The levator aponeurosis is attached to the following 4 structures (the "4 T's"):
- Trochlea
- Whitnall's Tubercle
- Tarsus
- Canthal Tendons
- The posterior division is Müller muscle (discussed below).
- The anterior division is the levator aponeurosis. It divides the lacrimal gland into the orbital and palpebral lobes. The levator aponeurosis is attached to the following 4 structures (the "4 T's"):
- The levator aponeurosis is firmly attached anteriorly to the eyelid skin, 3 mm superior to the eyelid margin. It is attached posteriorly to the anterior surface of the tarsus.
- The structure in the lower eyelid that corresponds to the levator aponeurosis is the capsulopalpebral fascia.
Whitnall's Ligament
- Whitnall's ligament is formed by a condensation of the superior rectus and levator muscles.
- It is attached to the trochlea fascia medially, and the fascia of the lacrimal gland (orbital lobe) laterally. The lateral attachment is at the level of the frontozygomatic suture, 10 mm superior to Whitnall's tubercle.
- It delineates the point where the levator palpebrae superioris muscle changes pull direction from anterior-posterior to superior-inferior.
- It demarcates the point where the levator palepebrae superior muscle "splits" into the levator aponeurosis and Müller muscle.
Tarsus
- The tarsus is composed of dense connective tissue, but is NOT cartilage.
- It is attached to the orbital margin by the medial and lateral palpebral ligaments and canthal tendons.
- Meibomian glands, which are holocrine sebaceous glands, are present in the tarsus and contribute to the oily layer of the tear film. There are more meibomian glands in the upper tarsus than the lower tarsus, which may explain why sebaceous cell carcinoma is more common in the upper eyelid.
Müller Muscle
- Müller muscle is a sympathetic-innervated muscle that contributes approximately 2 mm of action to eyelid opening.
- It originates from the levator palpebrae superioris at the level of Whitnall's ligament superiorly, and inserts at the superior aspect of the tarsus.
- The Müller muscle is the source of ptosis present in Horner's syndrome.
- Its lower-eyelid analogue is the inferior tarsal (capsulopalpebral) muscle, which originates from the inferior rectus and inserts at the inferior border of the inferior tarsus.
Conjunctiva
- The conjunctiva forms the posterior skin of the eyelid. Since there's a ton of information about the conjunctiva, I will put this information in a separate article.
Sample Questions (answers at the bottom of the page)
- What forms the gray line of the eyelid margin?
A. Mucocutaneous junction
B. Tarsus
C. Orbicularis oculi
D. Orbital septum
- Which muscle-innervation pair is CORRECT?
A. Horner's muscle - sympathetics
B. Levator palpebrae superioris - facial
C. Riolan's muscle - oculomotor
D. Capsulopalpebral muscle - sympathetics
- What structure separates the orbital and palpebral lobes of the lacrimal gland?
A. Whitnall's ligament
B. Levator aponeurosis
C. Orbital septum
D. Lateral palpebral ligament
- Which of the following glands are sebaceous glands?
A. Glands of Moll
B. Glands of Krause
C. Glands of Popoff
D. Glands of Zeis
Sample Question Answers
Orbital Anatomy
- A. The orbital floor is the only orbital wall that does not include the sphenoid bone.
- C. See #1.
- B. The superior transverse ligament is also called Whitnall's ligament. There are no firm attachments from Whitnall's ligament to Whitnall's tubercle.
- B. The frontal nerve (branch of V1), lacrimal nerve (branch of V1), trochlear nerve (CN IV), and superior ophthalmic vein lie outside the annulus of Zinn.
Eyelid Anatomy
- C. The gray line is formed by the muscle of Riolan. The muscle of Riolan is the most superficial portion of the orbicularis oculi muscle. It arises from the orbital segment of the orbicularis muscle.
- D. Horner's muscle is a portion of the palpebral segment of the orbicularis muscle, and is innervated by the facial (CN VII) nerve. The levator palpebrae superioris muscle is innervated by the oculomotor (CN III) nerve. Riolan's muscle is an extension of the orbital segment of the orbicularis muscle, and is also innervated by the facial (CN VII) nerve. The capsulopalpebral (or inferior tarsal muscle) is the sympathetically-innervated analogue of Müller's muscle in the lower eyelid.
- B. The levator aponeurosis separates the orbital and palpebral lobes of the lacrimal gland.
- D. The Zeis and meibomian glands are sebaceous glands. Zeis glands are present at the base of the cilia, and meibomian glands are present in the tarsus. The glands of Moll are apocrine sweat glands on the eyelid skin. The glands of Krause are accessory lacrimal glands that are present in the fornices. The glands of Popoff are accessory lacrimal glands that are present at the caruncle.
References and Additional Reading
- Basic and Clinical Science Course, Section 2: Fundamentals and Principles of Ophthalmology. American Academy of Ophthalmology, 2017-2018 edition.
- Basic and Clinical Science Course, Section 4: Ophthalmic Pathology and Intraocular Tumors. American Academy of Ophthalmology, 2017-2018 edition.
Do you have any suggestions on what else might be important to remember about orbit or eyelid anatomy that may show up on the OKAP? Do you have any tips for helping to remember all of this information? Do you have any requests for specific topics to cover? Leave a comment or contact us!